The impact of common comorbidities on shingles
Explore how common comorbidities can impact shingles risk, and why timely vaccination is essential to help protect your eligible patients.
Adverse events reporting and prescribing information can be found at the bottom of the page.
Healthcare professionals have been consulted by GSK and received honorarium.
Comorbidities are common amongst older adults1
In 2015, 54.0% of people aged over 65 had two or more conditions (multi-morbidity). By 2035, this is predicted to have risen to 67.8%.1
By age group, the prevalence of multi-morbidity was predicted at
- 52.8% for people aged 65-74
- 75.9% for those aged 75-84
- 90.5% for those above the age of 85.1

Your patients with common chronic conditions may be at increased risk of shingles, and shingles can disrupt the management of their condition2-11
Diabetes, chronic kidney disease (CKD) and cardiovascular conditions may increase an individual's risk of shingles, compared to the general population.2-9
When these patients develop shingles, it can disrupt their management of the condition.2,10
Diabetes
24%
of patients with previously well-controlled diabetes experienced increased HbA1c levels following shingles2*
What does this mean for a diabetic patient?
Haemoglobin A1C (HbA1c) is glycated haemoglobin. A high HbA1c means that the patient has too much sugar within their blood, and are therefore more likely to develop diabetes complications.23
Chronic Kidney Disease
36%
increased hazard of subsequent end-stage kidney disease in CKD patients who had shingles compared to those without10**
Adjusted HR: 1.36; 95% Cl: 1.09-1.70; p<0.01
(Total study population N = 4,999 patients and CKD patients with shingles N = 1,144, adults aged ≥ 18 years)
What does this mean for a patient with chronic kidney disease?
A hazard ratio is a statistical measure used to compare the risk of an event occurring in one group vs another over time. The adjusted hazard ratio (HR) of 1.36 means a CKD patient who had shingles in the duration of the study progressed to end stage kidney disease 36% faster than those with CKD who did not get shingles during that timeframe.10
The Shingles National Immunisation Programme can help to protect your patients, if they are eligible due to age or immunosuppression
Whilst diabetes, chronic kidney disease and cardiovascular conditions do not themselves deem an individual eligible for the shingles NIP, with these conditions becoming more prevalent with age, many of your patients will meet the age-based eligibility criteria.18-20***
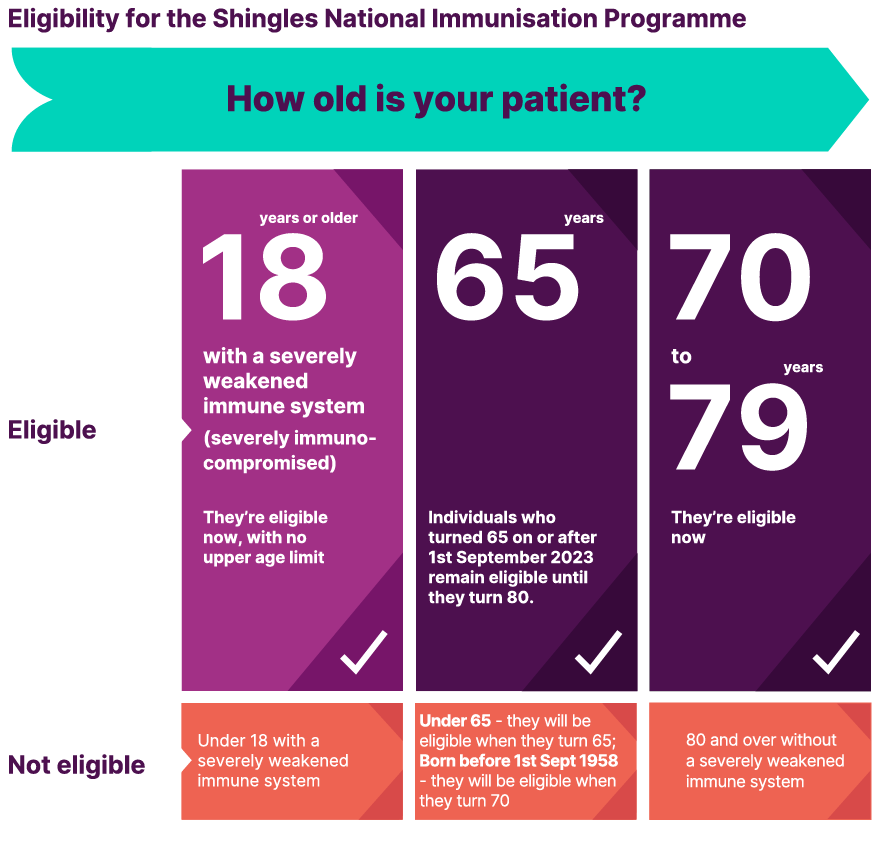
Which of your patients are eligible?
The eligible cohorts for the Shingles National Immunisation Programme in England & Wales are:
- Individuals aged ≥ 18 years who are severely immunocompromised (as defined in the Green Book)
- There is no upper age limit for this cohort
- Individuals who turned 65 on or after 1st September 2023
- Those born before 1st September 1958 will become eligible when they turn 70
- Remain eligible until their 80th birthday
- Individuals aged 70-79 years
- Remain eligible until their 80th birthday
The eligible cohorts for the Shingles National Immunisation Programme in Northern Ireland & Scotland are:
- Individuals aged ≥ 18 years who are severely immunocompromised (as defined in the Green Book)
- There is no upper age limit for this cohort
- Individuals aged 65 or 70 years on 1st September 2025
- Remain eligible until their 80th birthday
- This includes individuals that have already become eligible for the shingles vaccine due to their age (i.e. already 65 or 70 on the 1st September 2023 or 2024) and have not yet been vaccinated
- Those born before 2nd September 1957, will become eligible when they are aged 70 (on 1st September)
Your role in helping to protect your eligible patients
With patients becoming eligible for shingles vaccination each week, and many eligible patients remaining unvaccinated, a more proactive and systematic approach to vaccination is required.21
Use the drop downs below to understand how you can drive vaccination within your nation
- Proactively identify and invite your patients eligible for the Shingles National Immunisation Programme for their vaccination
- Organise dedicated shingles vaccination clinics – explore our content dedicated to breaking down eligible patient numbers into manageable amounts and simplifying the set up of a successful clinic
- Educate your patients on the importance of receiving both doses of the shingles vaccine22
Even if you are not administering shingles vaccination at your GP practice, you can support your patients by
- Informing your patients they are eligible for shingles vaccination
- Encourage your eligible patients to contact their Local Health Board and book their vaccination at their local Vaccination Centre
- Educate your patients on the importance of receiving both doses of the shingles vaccine22
Visit our webpage dedicated to the burden of shingles
* Using population and healthcare databases of Valencia Region (Spain), a retrospective cohort of all subjects 50 years and over was followed up between 2009 and 2014. The cohort consisted of 2,289,485 individuals, of whom 397,940 had diabetes. HZ incidence rate was 9.3 cases /1000 persons with diabetes-year (95% CI: 9.1–9 .4). Incidence increased with age in all groups. The risk of HZ increased in the diabetes group compared to the non-diabetes group (RR 1.2, 95% credibility interval [CrI] 1.17–1.22 ). Patients with diabetes utilized more health care resources due to their HZ episodes than patients without diabetes. In 24 % of well controlled patients with diabetes (HbA1C levels equal to or less than 6.5%), HbA1C increased after HZ.2
** A population-based matched cohort study (1:4) over the period of 1996 and 2008. Participants were identified from the Taiwan National Health Insurance Research Database. A total of 396 patients developed ESKD during the follow-up period, of whom 108 were from the shingles cohort and 288 from the comparison cohort. The mean follow up years were 3.0±2.3 years in the HZ cohort and 3.3±2.4 years in the comparison cohort. The log-rank test demonstrated that the shingles cohort had a significantly higher risk of developing ESKD than the comparison cohort (p=0.0071): incidence rates of ESKD per 100 person-years were 3.15 in the shingles cohort and 2.29 in the non-shingles cohort. HR was adjusted for sex, age, and comorbidities.10
*** Or if they meet the severely immunocompromised eligibility, as defined in the Green Book
References
- National Institute for Health and Care Research. Multi-morbidity predicted to increase in the UK over the next 20 years. Published March 2018. Available at: https://evidence.nihr.ac.uk/alert/multi-morbidity-predicted-to-increase-in-the-uk-over-the-next-20-years/
- Muñoz-Quiles C, López-Lacort M, Ampudia-Blasco FJ, et al. Risk and impact of herpes zoster on patients with diabetes: A population-based study, 2009–2014. Hum Vaccin Immunother. 2017;13(11):2606–11.
- Ke CC, Lai HC, Lin CH, et al. Increased risk of herpes zoster in diabetic patients comorbid with coronary artery disease and microvascular disorders: A Population-Based Study in Taiwan. PLoS One. 2016;11(1):e0146750.
- Icardi G, Francia F, Di Bartolo P, et al. Multi-disciplinary Consensus Statement Document Vaccinal prevention in adult patients with diabetes mellitus. J Prev Med Hyg. 2018;59(4):E249–56.
- Okamoto S, Hata A, Sadaoka K, et al. Comparison of varicella-zoster virus-specific immunity of patients with diabetes mellitus and healthy individuals. J Infect Dis. 2009;200(10):1606–10.
- Ishigami J, Matsushita K. Clinical epidemiology of infectious disease among patients with chronic kidney disease. Clin Exp Nephrol. 2019;23(4):437–47. Erratum in: Clin Exp Nephrol. 2019;23(5):723.
- Kato S, Chmielewski M, Honda H, et al. Aspects of immune dysfunction in end-stage renal disease. Clin J Am Soc Nephrol. 2008;3(5):1526–33.
- Watanabe R, Shirai T, Namkoong H, et al. Pyruvate controls the checkpoint inhibitor PD-L1 and suppresses T cell immunity. J Clin Invest. 2017;127(7):2725– 38.
- Marra F, Parhar K, Huang B, et al. Risk factors for herpes zoster infection: a meta- analysis. Open Forum Infect Dis. 2020;7(1):ofaa005.
- Lin SY, Liu JH, Yeh HC, et al. Association between herpes zoster and end stage renal disease entrance in chronic kidney disease patients: a population-based cohort study. Eur J Clin Microbiol Infect Dis. 2014;33(10):1809–15.
- Huang CT, Lee CY, Sung HY, et al. Association between diabetes mellitus and the risk of herpes zoster: a systematic review and meta-analysis. J Clin Endocrinol Metab. 2022;107(2):586–97.
- UKHSA Green Book: Shingles (herpes zoster): the green book chapter.
- UKHSA Shingles vaccination programme: expansion of SHINGRIX vaccine eligibility to all those who are severely immunosuppressed and aged 18 years and over. Published July 2025.
- Public Health Wales. Shingles – Information for health professionals.
- Shingles Immunisation Eligible groups – Public Health Scotland.
- Shingles Vaccination Programme 2025-26 SGHD CMO (2025) Chief Medical Officer for Scotland.
- Department of Health Northern Ireland. Shingles Vaccination Programme 2025/26. Published August 2025.
- Pouneh K. Fazeli, Hang Lee, Matthew L. Steinhauser. Aging is a powerful risk factor for type 2 diabetes mellitus independent of body mass index. Gerontology. 2020;66(2):209-210. doi: 1159/000501745.
- Public Health England. Diabetes Prevalence Model. Published September 2016.
- NHS England. Health Survey for England, 2022 Part 2. Published September 2024.
- UK Health Security Agency. Shingrix vaccine uptake report (adults eligible from September 2023 to August 2024 and vaccinated to the end of October 2024): England. Updated 31 October 2025.
- SHINGRIX Summary of Product Characteristics (United Kingdom).
- Diabetes UK. What is HBA1C? Available at: https://www.diabetes.org.uk/about-diabetes/looking-after-diabetes/hba1c. Last accessed March 2026.
March 2026 | PM-GB-HZU-WCNT-260001
For the SHINGRIX® (herpes zoster vaccine, recombinant, adjuvanted) prescribing information, click here.